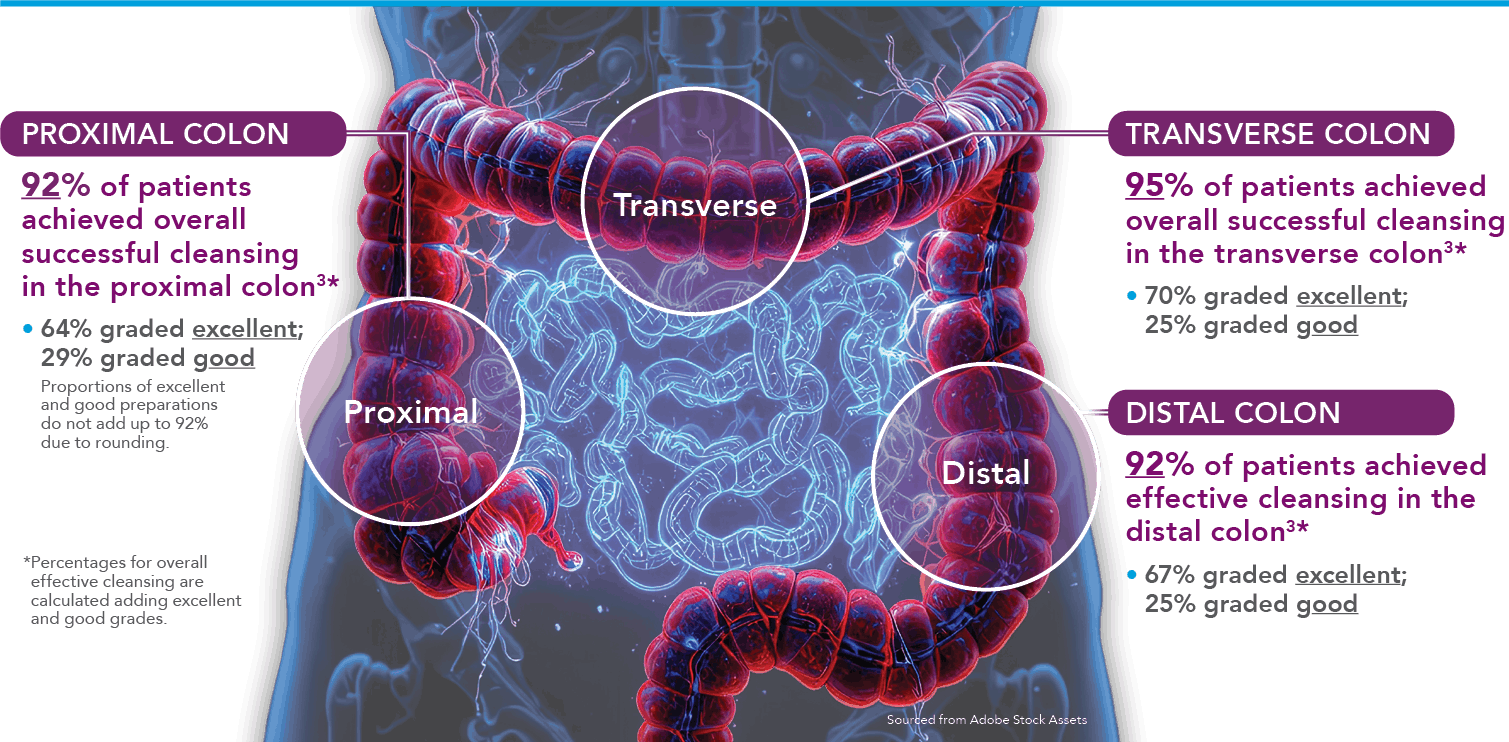
A prep is considered successful if it is good or excellent 2,3
- 97% agreement was seen between central and local readers3
SUTAB® Split-Dose Regimen†
Excellent
Good
Fair
Poor